Vitamin D: Getting the balance right
Pharmacy Magazine,
23 May 2019![]() 5 Min
5 Min
Pharmacy Magazine,
23 May 2019![]() 5 Min
5 Min
Pharmacy Magazine,
23 May 2019![]() 5 Min
5 Min

After reading this feature you should be able to:
• Discuss both the positive and negative effects of sunlight on the skin
• Explain the need for both UVA and UVB protection
• Raise awareness of the importance of checking skin moles for changes.
Sunlight is part of the electromagnetic spectrum and consists of roughly equal amounts of visible and infrared radiation and approximately 10 per cent ultraviolet (UV) radiation, which is responsible for the negative effects of sunlight. UV radiation is further divided into UVA, UVB and UVC rays.
Although more damaging to the skin, UVC radiation is filtered out by the ozone layer. UVB is responsible for sunburn and UVA for ageing – a useful mnemonic is UVBurning and UVAgeing – but both forms of radiation are known to be carcinogenic, hence the need to avoid overexposure and use sun protection measures.
UVB radiation produces vitamin D in the skin, which plays an important role in calcium and phosphorus homeostasis. As much as 90 per cent of a person’s vitamin D is obtained from exposure to sunlight. In recent years it has become apparent that vitamin D has numerous other roles in the body, including regulation of cell growth, neuromuscular and immune functions, as well as an anti-inflammatory role. Evidence also points to a possible protective role against certain cancers.
The term ‘vitamin D’ actually refers to two separate compounds: vitamin D3 (cholecalciferol) and vitamin D2 (ergocalciferol, which comes from plants). Upon hitting the skin, UVB radiation converts 7-dehydrocholesterol, which is present in cell membranes, into pre-cholecalciferol.
This pre-vitamin D is thermally unstable and converts into cholecalciferol and is taken up into the circulation. Prolonged exposure to sunlight does not lead to greater production of cholecalciferol but to the breakdown of both pre-vitamin D and cholecalciferol. Being lipid soluble, cholecalciferol is stored by adipocyte cells and has a half-life of up to two months.
Cholecalciferol is metabolised in the liver to 25-hydroxyvitamin D3 (25(OH)D) and then further broken down in the kidneys to 1,24-dihydroxyvitamin D3 (calcitriol). While calcitriol is the active metabolite, 25(OH)D is the main circulating form of vitamin D, which provides a reliable assessment of vitamin D stores, so is used when measuring vitamin D levels.
Production of vitamin D is highest when the sun reaches its peak in the sky around noon between March and September. However, this is also the time when the sun is likely to exert the most damage to the skin and eyes. Unfortunately, there is no good evidence to guide the duration of exposure to achieve sufficient levels of vitamin D as this depends on skin colour, the amount of skin exposed, time of day and latitude.
The NHS suggests that in the UK, people go outside daily (between April and the end of September) and expose their forearms, hands or lower legs for short periods between 11am and 3pm.
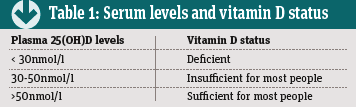
There is currently no clear consensus as to the optimal level of 25(OH)D. The National Osteoporosis Society has proposed the levels shown in Table 1 in relation to optimal bone health. Lack of vitamin D is recognised to be the most common worldwide nutritional deficiency and UK data indicates that 23 per cent of adults (19-64 years) and 21 per cent of those aged 65 years and over are vitamin D deficient.
The current reference nutritional intake (RNI) – i.e. the amount that will satisfy the needs of 97.5 per cent of the population – has been set at 10mcg per day for the UK population aged four years and upwards. This is particularly important for certain patient groups including those with darker skin types, people who for religious reasons wear long robes and head covered clothing, and the elderly living within institutions or who are hospitalised.
It is also important to note that the RNI assumes minimal sunshine exposure and that during the summer months, normal exposure to the sun will lead to increased vitamin D levels for most people.
Current guidelines suggest that routine testing of vitamin D is unnecessary, although identifying vitamin D deficiency is challenging because patients complain of non-specific symptoms such as aches and pains, tiredness and a general sense of being unwell. Testing is recommended in patients with a specific bone disease (e.g. osteomalacia, osteoporosis or Paget’s disease) if the person has experienced a fall.
There is no good evidence to guide the duration of exposure to the sun to achieve sufficient levels of vitamin D
The energy from UVB radiation is absorbed by chromophores (molecules or parts of molecules that absorb radiation) within cells. One specific chromophore is DNA and once irradiated, a series of compounds called cyclobutane pyrimidine dimers (CPDs) are formed, which constitute the major signs of DNA damage.
UVA radiation can also exert deleterious effects on the skin through the generation of reactive oxygen species (formerly termed free radicals), which damage DNA and various cellular proteins leading to signs of oxidative damage that may be important in mutagenesis.
Upon exposure to UVB radiation the skin increases the production of melanin from melanocyte cells and this leads to tanning. Melanin consists of two different forms, phaeomelanin, present in red haired individuals, and eumelanin, which is more prevalent in those with darker skins although, in practice, most skin types contain a higher proportion of eumelanin. The classification of skin types is based on the Fitzpatrick phototype as shown in Table 2.
Both UVA and UVB are capable of inducing tanning but UVA is more efficient (hence its use in sunbeds), whereas UVB is more likely to cause erythema (burning).
The melanin induced by UV radiation is transported along dendritic projections called melanosomes, which act to ‘cover’ epidermal cells, shielding them from the radiation. As a chromophore, melanin absorbs UV radiation, thus reducing its penetration through the epidermis.
Contrary to popular belief, individuals with higher value Fitzpatrick skin types do not possess more melanocytes. The difference in skin colour arises because of differences in melanogenic activity, the type of melanin produced, and the size and number of melanosomes.
For instance, black skin contains a higher proportion of eumelanin as well as a greater number and larger melanosomes than fair skin – a difference that helps to explain how black skin allows much less UV radiation to penetrate the epidermis compared to white skin.
In addition to the increased production of melanin, UV radiation also causes epidermal hyperplasia or thickening, which serves to increase the radiation path in the skin and hence decrease penetration of UV radiation.
• Sunburn is an inflammatory reaction caused by excessive exposure to UVB radiation
• SPF is best thought of as providing a relative, rather than absolute, measure of protection from the sun
• The most serious form of skin cancer is malignant melanoma and incidence is rising

Sunburn is an inflammatory reaction caused by excessive exposure to UVB radiation. The radiation increases the production of arachidonic acid in cell membranes, which is broken down to produce prostaglandin E2, which, in turn, causes vasodilation (hence the skin feels warm) and erythema (redness).
Sunburn can occur within three hours of UVB exposure and is characterised by erythema, oedema, tenderness, pain and skin that feels warm to the touch. In more severe cases there is blistering and systemic symptoms such as chills and fever. In the most severe cases patients may experience second-degree burns, dehydration and even death.
There are several treatments available for sunburn although a lack of convincing evidence and consensus for any specific therapy. The pain of sunburn can be relieved by using analgesics such as paracetamol or anti-inflammatory agents (e.g. ibuprofen).
NHS Direct advice for mild sunburn is to use a moisturising lotion or after sun product from a pharmacy. Such preparations help to cool the skin and relieve the feeling of tightness. Calamine lotion can also be used to relieve itching and soreness, although it is drying and rarely used for this purpose these days. Additional measures include applying cool (lukewarm) sponges to the skin or having a cool bath or shower.
Medical advice should be sought if small children and babies get burnt, particularly if the sunburn blisters or a rash develops.
Sunscreens contain two different types of chemical agents:
• Chemical absorbers
• Physical blockers.
Chemical UV absorbers are the more commonly employed agents in sunscreens and convert UVB radiation into heat, which is then released from the skin. The majority of the sunscreen preparations available to purchase contain derivatives of one of the following: aminobenzoates, anthranilates, benzophenones, cinnamates and salicylates.
Physical blockers are mainly insoluble pigments like zinc oxide or titanium dioxide. These act primarily by forming a non-transparent film on the skin surface, which scatters and reflects UV radiation, providing a total block of both UVA and UVB rays. Formulations containing these agents are effective but by nature thick, conspicuous and cosmetically unacceptable to many individuals.

The most commonly used term to describe the protection offered against burning from UVB radiation in a sunscreen is the sun protection factor (SPF). The SPF is used as a measure of how much longer a person can stay in the sun without burning. For example, if someone normally burns after 20 minutes, applying a sunscreen with an SPF of 15 means that they can stay 15 times longer (i.e. 300 minutes or five hours) before they would burn.
This is a common misconception, however, because although increased time in the sun increases exposure, the level of burning experienced varies with the intensity of solar radiation, which itself depends on several other factors. For instance, exposure at 9am would need to be longer than at midday to achieve the same intensity of radiation because of the low angle of the sun.
The amount of UV radiation impacting on skin varies depending on the season, latitude and altitude, as well as reflection from sand, water or snow. The SPF is best thought of as providing a relative, rather than absolute, measure of protection. The degree of UVB radiation blocked by sunscreen products is non-linear, as shown in Table 3.
Although UVA radiation does not lead to burning, it can cause skin ageing, which leads to the development of wrinkles and is carcinogenic. In addition, UVA, but not UVB, can penetrate through glass. The protection against UVA is measured using a star rating system from one to five (highest) as shown in Table 4. Patients should aim to use a broad spectrum agent (i.e. a product which has a high SPF and UVA rating).
A product with a SPF of 15 and 5-star UVA rating is sufficient for most people but for those whose skin burns very easily, SPF 30 or SPF 50 would be more appropriate. A high SPF sunscreen should also be used on babies and young children. Patients with Fitzpatrick skin type VI would not normally need a sunscreen unless they have photosensitivity or abnormal pigmentation.
Loose fitting garments that are deeper in colour and close weave are more beneficial in the sun
Sunburn often arises in patients who use a sunscreen because they have failed to apply sufficient amounts of the product. General advice includes the following:
• Apply the sunscreen to dry skin roughly 30 minutes before going out in the sun
• Re-apply every two hours or more frequently if washed, rubbed or sweated off. This also applies to products labelled as ‘water resistant’
• Ideally, the amount of sunscreen required for a whole adult body would be 35ml or around six to eight teaspoons.
Clothing is another important protective measure and loose fitting garments that are deeper in colour and close weave are more beneficial in the sun. A quick guide to the level of sun protection offered by a garment can be gauged by holding it up to the light. If it is difficult to see through the clothing, it offers more protection. Wet clothing – especially cotton clothes – offers less protection.
Wide-brimmed hats will offer protection for the whole face and head, and sunglasses are necessary to protect the eyes. Products bearing the CE mark and labelled as UV 400, or which offer 100 per cent UV protection, are the ones to recommend.
The most serious form of skin cancer is malignant melanoma. According to Cancer Research UK, there were nearly 16,000 new cases of melanoma in 2015 and it was the fifth commonest cause of cancer.
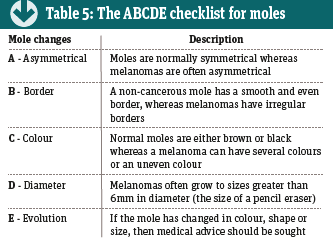
Eighty-six per cent of cases are due to overexposure to UV radiation. Roughly half of all melanomas arise from existing moles, so it is important that patients regularly inspect their moles for changes. The ABCDE mole check has been used for several years and is described in Table 5.
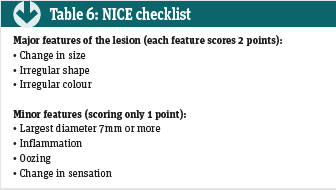
In addition to the ABCDE checklist, NICE has identified a further seven-point checklist that healthcare professionals should use when considering referring a patient with a suspected melanoma (see Table 6). All patients scoring three or more on this checklist should be referred under the twoweek cancer referral pathway.
 Cholecalciferol is metabolised in the liver to 25-hydroxyvitamin D3 (25(OH)D) and then further broken down in the kidneys to 1,24-dihydroxyvitamin D3 (calcitriol). While calcitriol is the active metabolite, 25(OH)D is the main circulating form of vitamin D, which provides a reliable assessment of vitamin D stores, so is used when measuring vitamin D levels.
Cholecalciferol is metabolised in the liver to 25-hydroxyvitamin D3 (25(OH)D) and then further broken down in the kidneys to 1,24-dihydroxyvitamin D3 (calcitriol). While calcitriol is the active metabolite, 25(OH)D is the main circulating form of vitamin D, which provides a reliable assessment of vitamin D stores, so is used when measuring vitamin D levels.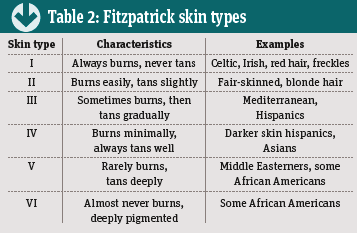 There is currently no clear consensus as to the optimal level of 25(OH)D. The National Osteoporosis Society has proposed the levels shown in Table 1 in relation to optimal bone health. Lack of vitamin D is recognised to be the most common worldwide nutritional deficiency and UK data indicates that 23 per cent of adults (19-64 years) and 21 per cent of those aged 65 years and over are vitamin D deficient.
There is currently no clear consensus as to the optimal level of 25(OH)D. The National Osteoporosis Society has proposed the levels shown in Table 1 in relation to optimal bone health. Lack of vitamin D is recognised to be the most common worldwide nutritional deficiency and UK data indicates that 23 per cent of adults (19-64 years) and 21 per cent of those aged 65 years and over are vitamin D deficient.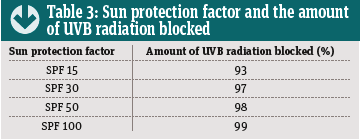 This is a common misconception, however, because although increased time in the sun increases exposure, the level of burning experienced varies with the intensity of solar radiation, which itself depends on several other factors. For instance, exposure at 9am would need to be longer than at midday to achieve the same intensity of radiation because of the low angle of the sun.
This is a common misconception, however, because although increased time in the sun increases exposure, the level of burning experienced varies with the intensity of solar radiation, which itself depends on several other factors. For instance, exposure at 9am would need to be longer than at midday to achieve the same intensity of radiation because of the low angle of the sun.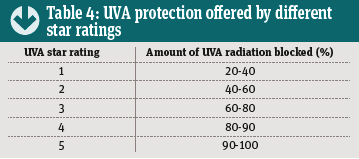 Although UVA radiation does not lead to burning, it can cause skin ageing, which leads to the development of wrinkles and is carcinogenic. In addition, UVA, but not UVB, can penetrate through glass. The protection against UVA is measured using a star rating system from one to five (highest) as shown in Table 4. Patients should aim to use a broad spectrum agent (i.e. a product which has a high SPF and UVA rating).
Although UVA radiation does not lead to burning, it can cause skin ageing, which leads to the development of wrinkles and is carcinogenic. In addition, UVA, but not UVB, can penetrate through glass. The protection against UVA is measured using a star rating system from one to five (highest) as shown in Table 4. Patients should aim to use a broad spectrum agent (i.e. a product which has a high SPF and UVA rating).